Nutrition Tip #2 Tomatoes & Cancer
Reply
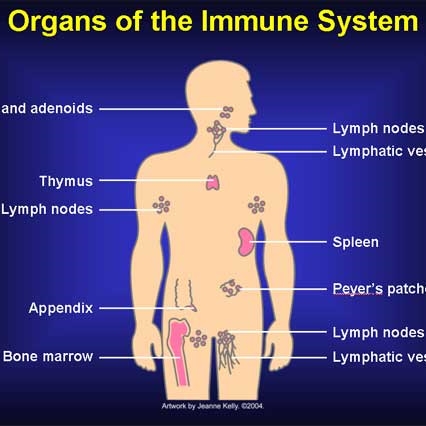 A role of our immune system in preventing cancer has been postulated for over 50 years. However, it has only been recently that researchers have been able to begin to unravel the complexity of the immune system’s role in cancer and begin to harness the immune system to fight cancer.
A role of our immune system in preventing cancer has been postulated for over 50 years. However, it has only been recently that researchers have been able to begin to unravel the complexity of the immune system’s role in cancer and begin to harness the immune system to fight cancer.
Present research suggests that from time to time we may all be developing cancerous cells which are kept in check by our immune systems. One of the mysteries of advanced cancer has been why some cancerous cells are able to escape from immune suppression so that the immune system does not always effectively attack one’s cancer. Under the microscope cancer-fighting T-lymphocytes can be seen surrounding cancer cells but not killing them. One reason that has been discovered is that some cancers may produce signals that tell the “T” cells to go into a kind of immune hibernation. Newly developed drugs block these cancer produced signals and, in certain cancers, have led to dramatic cancer shrinkage.
Normally T cells have a limited life span and die via a normal phenomena known as apoptosis. A new class of drugs called “programmed death” or PD-1 inhibitors tells T cells to stick around longer and not die so that they can more effectively fight cancers. In yet another strategy, pioneered locally at the National Cancer Institute, T cells are removed from tumors, genetically re-engineered to make them better cancer fighters, and then re-infused back into the patient. The advantage of this type of therapy is that the new T cells can take up residence in the body and be around for a long time to perpetually keep the cancer on the run.
Researchers are working on combinations of these different strategies and trying to figure out how to prevent unintended serious side effects, such as the activated and aggressive cancer fighting T cells not attacking normal tissues. Some of these strategies require individualizing treatments for each cancer, and each individual, and thus are not presently practical on a large scale. The field is in its infancy but nonetheless has been making dramatic progress. In our own practice we have seen a few patients begin to benefit from these new therapies. Many of the researchers have been working on this for their entire careers. They, and the institutions that have supported them, deserve a lot of thanks for their efforts that hopefully will eventually lead to a new era in cancer treatment.
 On January 10, 2014, the Centers for Medicare & Medicaid Services (CMS) and the state of Maryland jointly announced a new initiative to “modernize Maryland’s unique All-Payor rate-setting system for hospital services that will improve patient health and reduce costs.” Sounds great, “improve patient health and reduce costs,” but what is the reality? Well, first one has to understand the uniqueness of the present system in Maryland.
On January 10, 2014, the Centers for Medicare & Medicaid Services (CMS) and the state of Maryland jointly announced a new initiative to “modernize Maryland’s unique All-Payor rate-setting system for hospital services that will improve patient health and reduce costs.” Sounds great, “improve patient health and reduce costs,” but what is the reality? Well, first one has to understand the uniqueness of the present system in Maryland.
Four decades ago the state was faced with a number of disturbing trends. Hospital costs in Maryland were rising much faster than the national average and Maryland hospitals with high levels of uninsured patients were on the verge of bankruptcy. In other states, such as California, hospitals were said to be engaged in rampant “cost shifting” and “patient dumping” whereby patients without insurance were being refused by profitable hospitals. Around this time Medicare was starting to come up with its own solutions.
Not wanting to cede control to the emerging payment policies of the federal government, the state developed its own unique “All-Payor” hospital system and convinced the federal government to issue Maryland a waiver from the Medicare payment system. To keep hospital costs from exploding, a Hospital Services Cost Review Commission was created; and all insurance companies were required to pay hospitals the same rate mandated by the commission rather than negotiated by the individual hospitals and insurance companies. The rates paid could differ from hospital to hospital, depending on its mix of uninsured. From a social policy point of view, the program was successful. It kept hospitals solvent, provided a dependable method for hospitals to get paid, and obviated the need for public hospitals for the uninsured.
For 36 years Maryland remained the only state in the union to have been granted and kept its Medicare exemption. However, as health care evolved, the Maryland system did not. With health care shifting increasingly to an outpatient setting, the inpatient Maryland model no longer was capable of keeping global health costs down for a number of reasons, many self-inflicted.
State agencies allowed large hospital conglomerates such as Medstar to take over multiple smaller hospitals and then get into the business of running outpatient services while charging and getting paid higher inpatient rates. Meanwhile, the Cost Review Commission continued to approve costly additions to hospitals offering duplicate services even as hospital occupancy rates were falling. Finally, insurance companies such as United (annual profits of over $5 billion) were allowed to maximize their profits in the face of increasing hospital costs by cutting reimbursements to experienced primary care practices to 20% or less than Medicare. Add to that the debacle of the Maryland Health Exchange, the premise that the exchange would foster competition among health insurers was laid bare when Cigna and Aetna could not be convinced or cajoled to participate, essentially leaving just United, Carefirst, and Kaiser to participate.
To keep its cherished waiver Maryland has agreed to require Maryland hospitals to keep annual increases for both inpatient and outpatient services not to exceed 3.58% over the next five years and thereby generate $330 million in Medicare savings over a five-year performance period. Also the hospitals will need to initiate programs to improve their quality ratings. In theory, if Maryland can’t pull this off, they will then lose the waiver (unless the politicians get involved as they likely did this time around).
So where does that leave us? At the end of the day, we are left with a system in Maryland essentially dominated by a couple of monolithic health care companies (United and Carefirst) with little competition, huge hospital systems which for years have gotten used to being fed a rich diet doled out by order of the state, and a decimated primary care system.
The likely scenario will be an acceleration of present trends, more consolidation and less competition, doctors with years of training and experience replaced by mid levels (nurse practitioners and physician assistants just graduated from college), registered nurses with years of training replaced by medical assistants with weeks of training, quality assessed by bureaucratic checklists, and cost savings to pay for all those new shiny buildings coming from layoffs of the most important asset – experienced people.
 Some of our patients have asked about taking Biotin to treat hair loss and brittle nails. I asked our nutritionist Rick to comment:
Some of our patients have asked about taking Biotin to treat hair loss and brittle nails. I asked our nutritionist Rick to comment:
Biotin deficiency causes structural changes in the hair and nails. However, biotin deficiency is rare, because your gut bacteria actually make it. The people most likely to suffer from biotin deficiency include: those taking antibiotics for long periods of time; people eating raw egg white; and possibly anti-seizure medications. There’s no evidence that people with hair loss or changes in hair quality have benefited from biotin supplements. Nails may be another story. Human studies found that the overwhelming majority of women with brittle fingernails who took biotin (2.5 milligrams of biotin each day for up to 6 months) saw improvements in nail quality (i.e., less splitting and cracking). However, none of these were ‘controlled’ trials, so the jury is still out.
Good food sources include whole wheat bread, avocado, raspberries, and cauliflower.
Rick Weissinger, MS, RD, LDN, CPT
Author, WHAT THE EXPERTS SAY ABOUT FOOD AND CANCER
Co-author, NUTRITION GUIDE FOR CLINICIANS, editions 1 and 2
Web site: www.idomnt.com
Phone: (301) 525-9078